History:
A 38-year-old Caucasian female with a history of a facial dog bite resulting in avulsion of 30% of her lower lip presented to the plastic surgery clinic with concerns of unacceptable lip appearance and oral incompetence. Initial closure was deemed inadequate, and she underwent an Abbe flap closure followed by division of the Abbe the flap by OMFS four and five months respectively after primary injury. She desired revision for better appearance and to improve her oral competence.
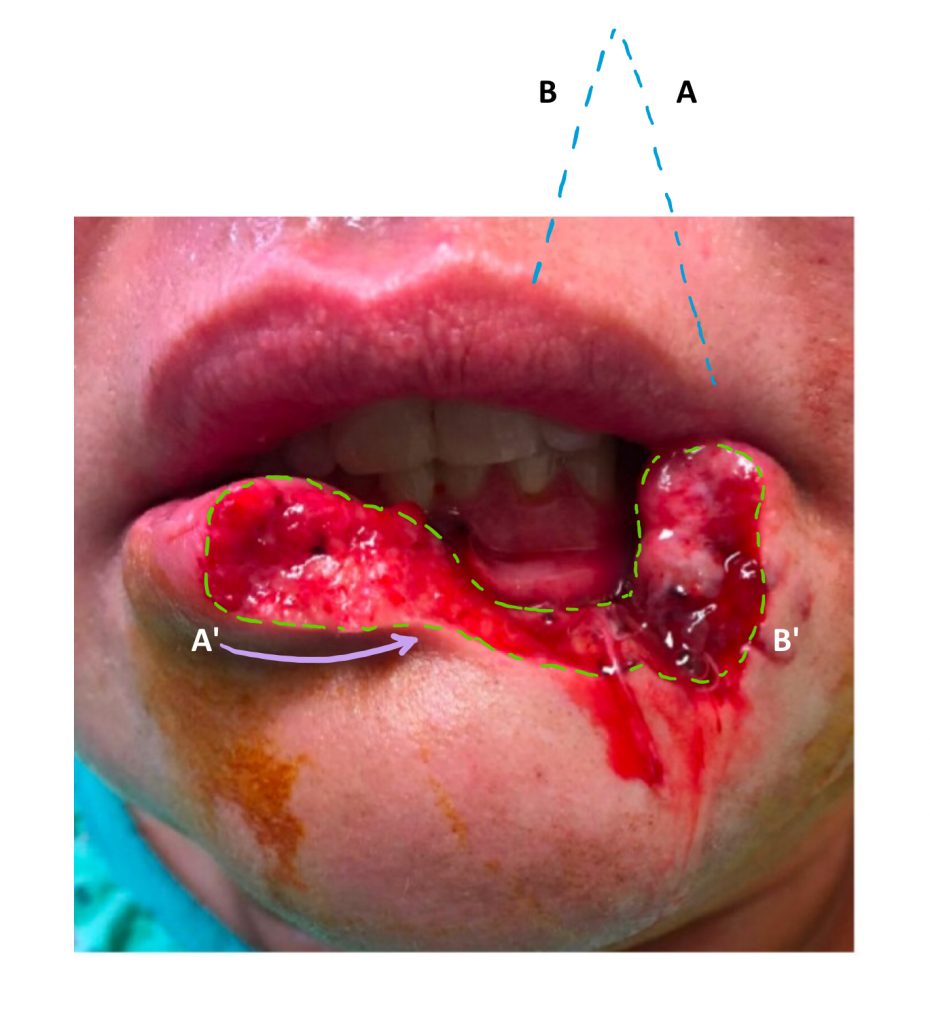
Initial injury showing avulsion of the lower lip including the vermillion border. Blue dotted line denotes the approximate location of the Abbe flap. The purple arrow indicates advancement of tissue medially, with A-A’ and B-B’ denoting match points between the flap and inferior lip. The green dotted line outlines tissue that was further debrided.
Findings:
Eight months later, there was a step-off deformity of the upper lip with malalignment of the vermillion border, decreased fullness of lower lip and hypertrophic scarring leading to puckering suggestive of a mal-positioned orbicularis muscle.

Pre-operative photo showing a step off deformity and mal-alignment of the vermillion border in the upper lip in Abbe flap donor area. Scarring and lack of volume in lower lip.
Follow Up:
The patient was seen 6 weeks post operatively with no complications. She returned to the clinic five months post operatively desiring additional fat grafting. Additional fat grafting was performed, leading to a satisfactory final result.

A post-operative photo showing improved step off deformity, enhanced alignment of the vermillion border, and improvement in hypertrophic scarring.
