History:
24-year-old right hand dominant male with no significant past medical history presented with a lacerated right index finger nail bed and distal fingertip with a minimally displaced distal phalanx tuft fracture after sticking his hand in a fan blade at a cattle show earlier that day.

Fig.1. Right hand, laceration of 2nd finger

Fig.2. Xray of right hand. Minimally displaced tuft fracture of 2nd distal phalanx
Follow Up:
The dressings remained occlusive for 48 hours. After this, the patient was told to gently clean with warm soapy water and perform daily dressing changes with bacitracin, xeroform, gauze, and kerlix. The patient was also allow the xeroform to soak to make it easier to remove. The cage splint was used for comfort with a tuft fracture. Arm elevation was encouraged to minimize pain and swelling –any swelling in the fingers causes a great increase in throbbing pain. Tylenol and ibuprofen was be used to pain control. Showers were allowed, but no submerging or soaking in water for two weeks. No lifting for over 10lbs for two weeks.
The patient was seen two weeks later in clinic. At the time, the digit was demonstrating appropriate healing. Recommended continuing bacitracin and dressings to protect from outside environment and cap splint for comfort. He was released to his manual job per his abilities.

Fig.3. Two week follow up
‘
He was seen once again one month after the initial visit. New nail growth was seen. There was minimal pain to the distal fingertip and the wound was healed. He was able to work without limitations. Discussed the growth cycles of the nail and that it would take about one year to fully know what the nail will look like.
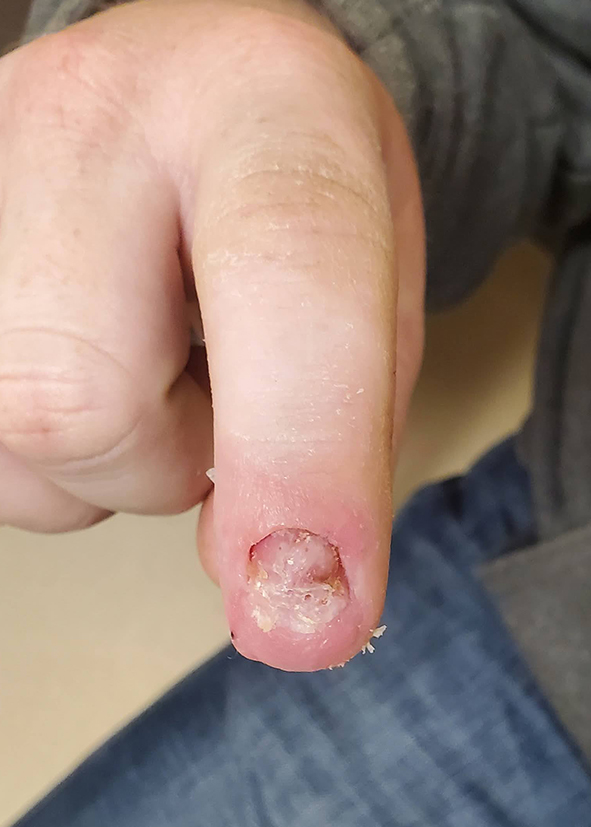
Fig.4. Six week follow up
–
