Findings:
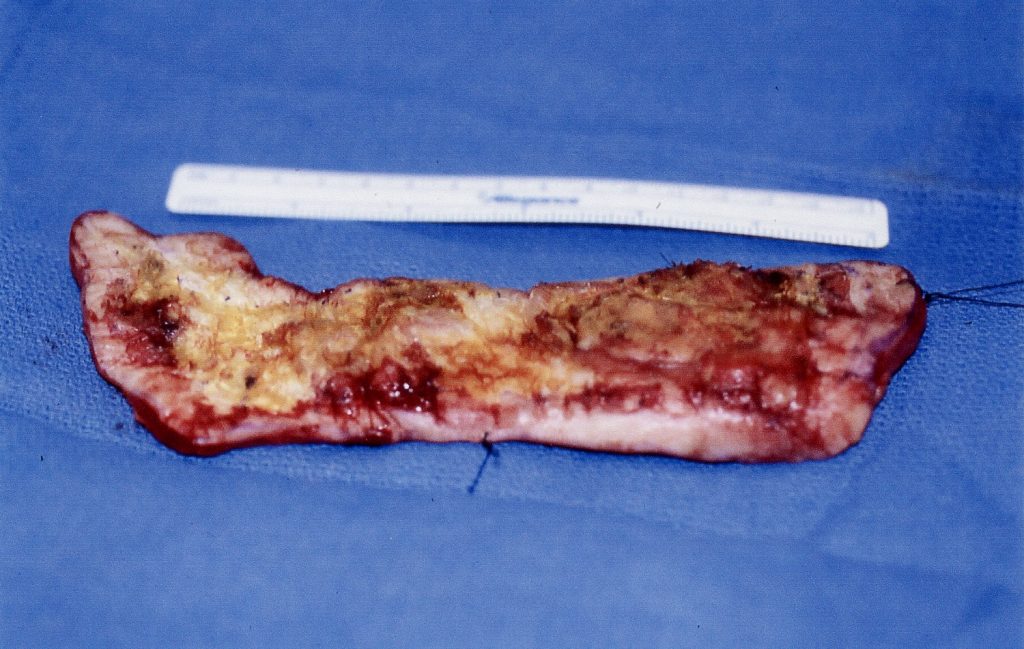
49 year old man who ha severely scarred skin everywhere except on his hands and feet. In the left popliteal fossa and extending vertically up and down, there is a 22 X 6 cm area which is partially ulcerated partially keratinized. Biopsy has shown verrucous carcinoma. There are no palpable lymph nodes in the popliteal fossa or groin.

Treatment:
With the patient prone and under local anesthesia with .5% Lidocaine local anesthesia, the tumor was resected with a 10 mm lateral margin and including the fascia in the deep margin. After careful hemostasis, the wound was packed with saline gauze and an elastic wrap while waiting for the pathology report. The patient was discharged on oral pain medication.
Pathology showed margins free of tumor and the wound was closed 48 hours after the resection. A split thickness skin graft, 10/1000 inch thick was taken from the left forearm, meshed , expanded and sutured in place with 4.0 chromic gut. Xeroform gauze, dry gauze and an elastic wrap was used to provide a pressure dressing.
Follow Up:
One week following skin grafting there was complete take of the graft. Three weeks later the area was fully epithelialized.

