Diagnosis:
Complex laceration of upper lip including vermillion border.

Fig. 1. This image illustrates the wound on presentation. Complex laceration of upper lip including vermillion border
Treatment:
The patient was placed in the supine position with good lighting. The vermillion border on both sides of the wound was marked with a surgical marker prior to infiltration with local anesthetic. The wound was infiltrated locally with 5cc of 1% xylocaine with epinephrine (1:100000). Direct infiltration was chosen over an infra-orbital nerve block as the wound was central and was not very large. The wound was irrigated thoroughly with 1L of sterile saline and examined for depth and involvement of surrounding structures. As aforementioned, the orbicularis oris muscle was intact and did not require repair. The oral mucosa was also not violated which was also consistent with the prior exam. The vermillion border was first using the prior surgical markings and a 7.0 prolene simple interrupted suture. The skin along the right philtral column and along the dry lip was also closed using simple interrupted 7.0 prolene sutures. At the transition point of the wet lip and dry lip, a simple interrupted 5.0 chromic gut suture was used. Simple interrupted 5.0 chromic gut sutures were also used to close the remainder of the wet lip laceration. Bacitracin was applied to the wound and the patient was instructed to apply Bacitracin ointment twice daily until follow up. She was also instructed to avoid sun exposure and use SPF-30 or higher lotion if exposed to sun for the next year. This was done in order to decrease the chance of differential pigmentation of her scar. She was scheduled for follow up in 1 week for suture removal. On follow up visit, her wound was healing well, the sutures were removed, and the patient was instructed to apply Vaseline to the healed laceration until the lip was no longer crusting.
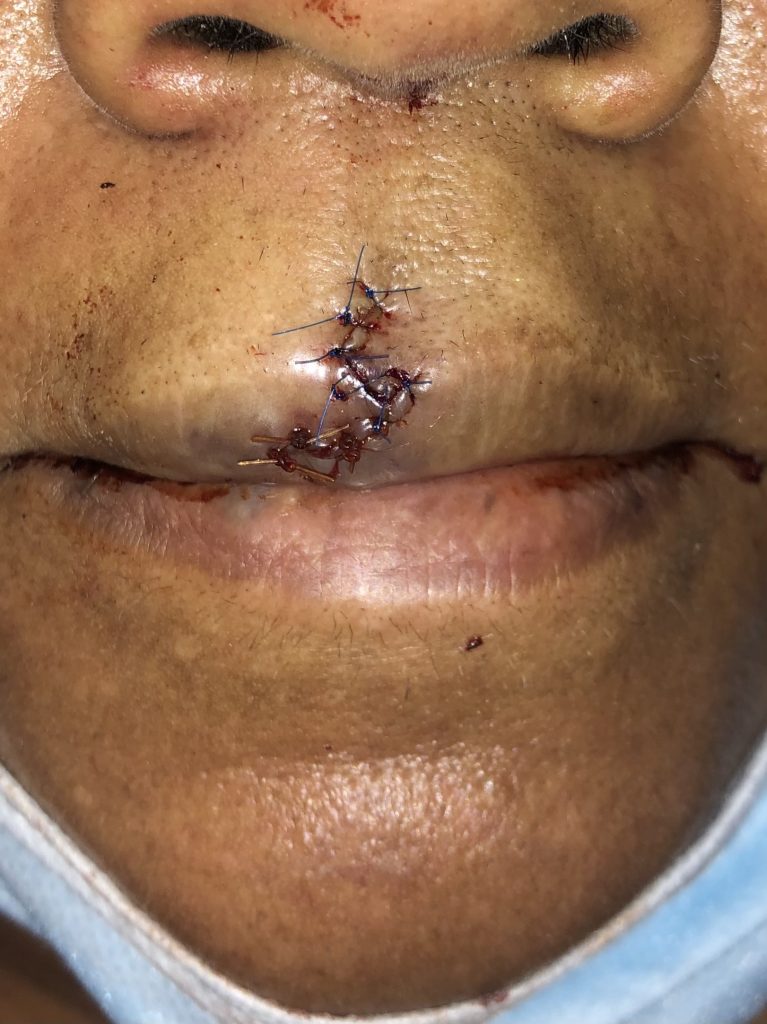
Fig. 2. This image illustrates the wound after placing the sutures. The patient was scheduled for follow up in 1 week for suture removal.
Follow Up:

Fig. 3. The healing wound after removal of the sutures and imaged during a follow up visit.
