Findings:
43 year old woman in a wheel chair, who is alert and oriented and with a healthy appearance outside of a T10 paraplegia. She has no bladder control and uses a urethral catheter. She has no sensory or motor function below the T10 level. Over the right ischium there is a 2 cm opening surrounded by callused tissue. There is no evidence of invasive infection. Probing with a metal probe reveals exposed bone without periosteum and an ulcer that is 8 cm deep and surrounding the ischial tubercle.

Fig. 1. Right ischial pressure sore.
Treatment:
The patient was admitted the day of surgery and the operation was done under general anesthesia (the sometimes uncontrollable spasms made local anesthesia a less attractive option). The ulcer cavity was first stained with methylene blue and then excised in a pseudotumor fashion. An osteotome was used to excise infected bone and lower the ischium by 11/2 cm. An inferiorly based rotation flap was first outlined and elevated. Then a gluteus maximus flap was then elevated and transposed in place to cover the osteotomized ischium. Finally the rotation flap was moved to cover the skin defect. Two large suction drains were used.
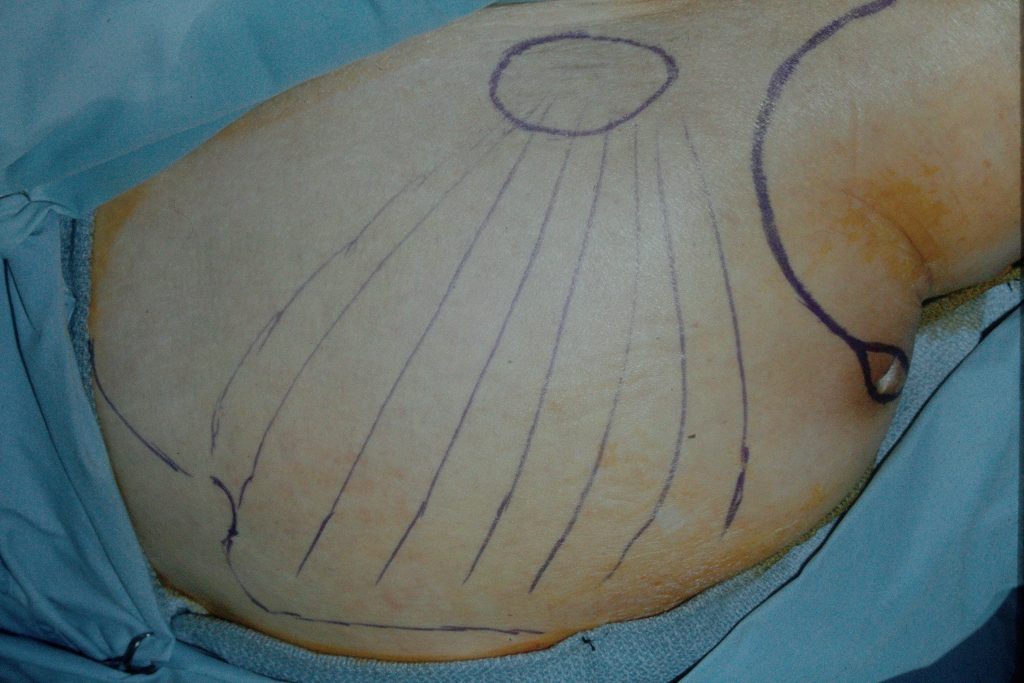
Fig. 2. Drawings outlining the operation with an inferiorly based rotation flap and a gluteus maximus muscle flap.
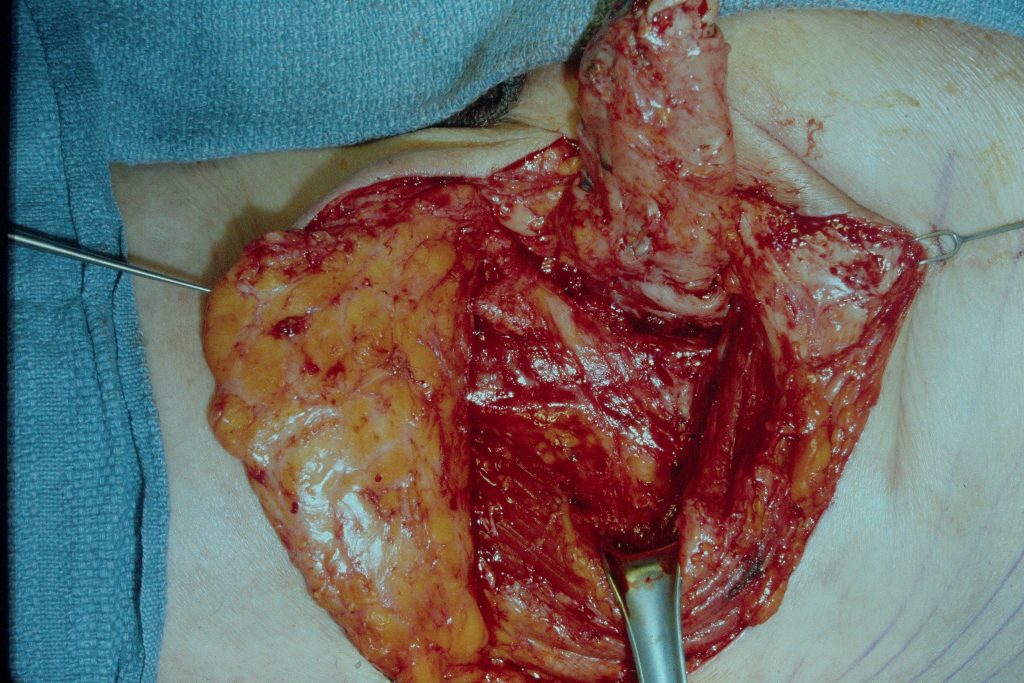
Fig.3. Both flaps elevated after resection of the pressure sore.

Fig. 4. The sutured wound.
