Findings:
Upon examination the patient had non-palpable pedal pulses, forefoot crepitus, superficial skin necrosis, malodorous, purulent draining wound, and a loss of protective sensation. Diagnostic imaging, vitals, and labs confirmed septic necrotizing fasciitis infection. Furthermore, an arterial duplex ultrasound exhibited significant tibial arterial stenosis.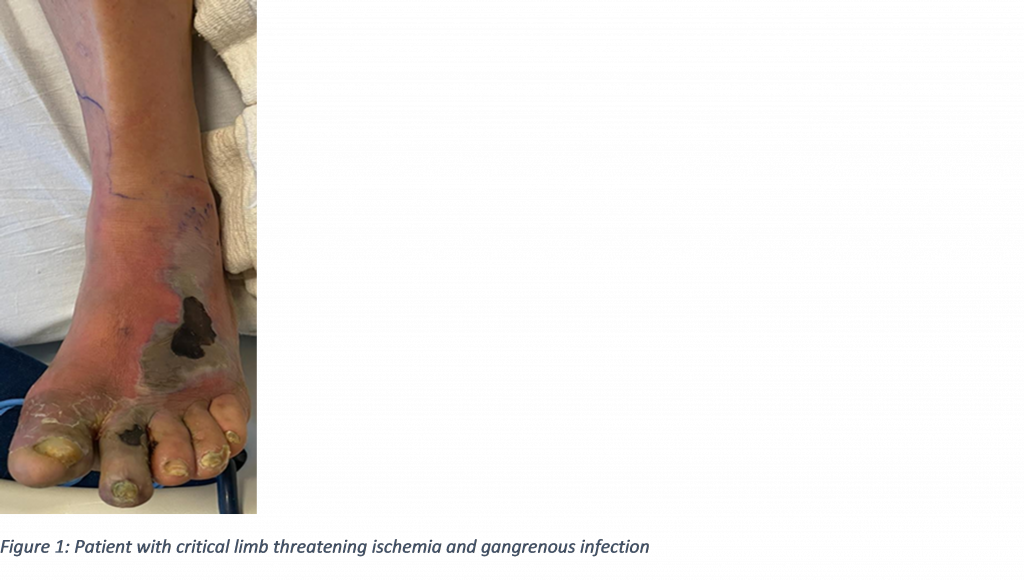
Treatment:
Despite lack of pedal pulses, patient received an immediate partial first ray amputation with midfoot debridement of nonviable tissue. Without prompt open amputation the patient would have remained septic in limb and life-threatening context. During admission patient received an angiogram with angioplasty of tibial vessels to provided patent blood inflow to foot. Antibiotic regimen was selected based off intra-operative cultures. Endocrinology was brought on board for glycemic control and long-term insulin management. With blood sugar control and improved vascular inflow, the patient was brought back into the operating room for a transmetatarsal amputation with application of a collagen-based graft product to expedite healing.

