History:
A 81-year-old woman, with history of hypertension, was referred to our hospital from her primary care physician. She developed a small wound on her left lower leg after scratching two weeks ago. After that, the wound became larger and deeper, and she couldn’t walk because of severe pain.
Treatment:
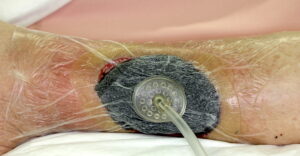
After hospitalization, culture from the deep area of the ulcer was taken and antibiotics treatment was started. Antibiotics was performed empirically fist and changed to the most appropriate based on the culture results. ABI was normal, deep venous thrombosis was excluded by ultrasound and there was no indication for varix surgery. We ordered her bed rest and applied an elastic bandage on her lower leg. Her wound was washed and covered with moist wound dressing every day. 5 days later, sharp debridement was performed under general anesthesia. Necrotic and infectious tissue including fascia was fully debrided, and negative pressure wound therapy (3M™ ActiV.A.C.™ Therapy System; 3M) was applied. After three weeks, her wound was covered with good granulation tissue, and a mesh skin graft was performed in the operating room. Her wound healed completely.


Follow Up:
After six years, she could walk with compression stocking and there was no recurrence.
