Findings:
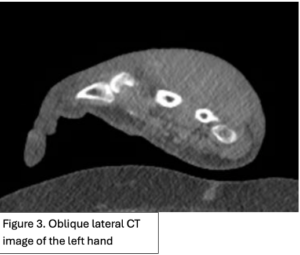
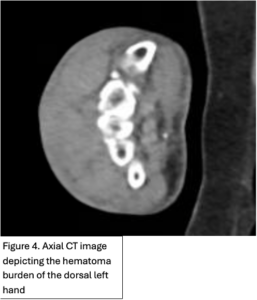
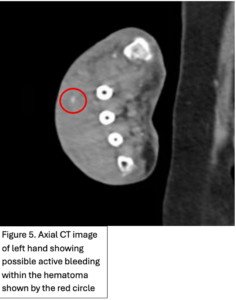
Figure 1. Left dorsal hand demonstrating significant soft tissue edema extending to tips of the digits. Ecchymosis of left first and fifth digits, dorsum of hand and wrist, and distal posterior antebrachium. Blisters evident on dorsum of left hand and between second and third digits. Figure 2. X-ray of the dorsal left hand and wrist demonstrating minimally displaced triquetral fracture. A subtle fracture through the dorsal edge of the triquetrum could not be excluded. Figure 3. and Figure 4. Illustrate the burden of the hematoma. Figure 5. Appreciates a focus of enhancement suggesting bleeding or possible dystrophic calcification, however with clinical correlation it was determined more likely to be an active bleed
.

Follow Up:
Examination at 1 month follow-up revealed a 3 x 3 cm healing wound of the dorsal aspect of the left hand with granulation tissue present in the base (Figure 6). There was no evidence of infection or exposure of vital structures such as the extensor tendons. The hand was neurovascularly intact. The patient endorsed intact sensation to the dorsum of the hand. There was marked stiffness appreciated on physical exam with significant swelling around the digits causing decreased range of motion. Integument was otherwise unremarkable. Daily Xeroform dressings were recommended for healing by secondary intention given the excellent granulation tissue already present at the superficial wound base (1). She was taken to hand therapy for edema control and range of motion exercises. She was instructed to follow-up in office 4 weeks later to re-evaluate wound healing progression and range of motion of the fingers.

Due to declining clinical condition as well as various social barriers, patient was initially lost to follow up and did not receive hand therapy. Hand therapy is imperative during recovery of hand injuries to aid in preventing joint contractures and maintain motion of the fingers. Examination at 6 month s/p hematoma evacuation showed a fully healed left dorsal hand, with a 5 cm scar (Figure 7.).

