Findings:
On exam, 4 cm long, deep laceration to the left chin, with exposed mentalis muscle. The laceration was deep but with no intraoral component. There was no loss of teeth or evidence of facial fractures.


Figure 1-2. Show left chin laceration.
Treatment:
The patient was placed in the supine position with good lighting. The wound was copiously irrigated with saline and betadine solution. In the muscle, 4-0 Monocryl sutures were used. In the superficial layer, 6-0 Monocryl dermal sutures were used to approximate the dermal edges. 6-0 Prolene interrupted sutures were used for the best skin approximation. Bacitracin was applied to the wound and the patient was instructed to apply Bacitracin ointment twice daily until follow up. He was also instructed to avoid sun exposure and use SPF-30 or higher lotion if exposed to sun for the next year. This was done in order to decrease the risk of hyper pigmentation of her scar. He was scheduled for follow up in 1 week for suture removal. He received 5 days of prophylactic antibiotics. At the follow up visit, his wound was healing well, the sutures were removed, and the patient was instructed to apply Vaseline to the healed laceration until there was no more crusting.


Figure 3-4. Show repaired left chin laceration.
Follow Up:
One week for removal of non-resorbable sutures, followed by 1 month follow up for healing. Additional follow ups as needed depending on scar maturation and healing.
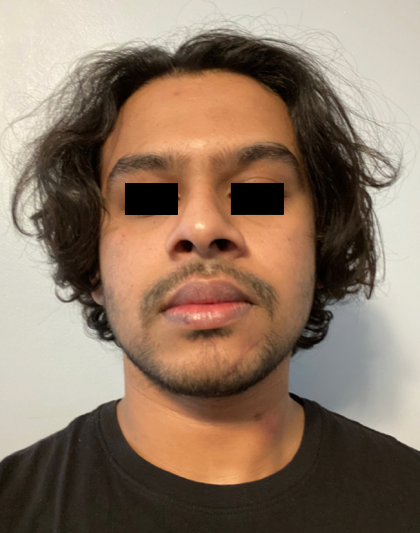
Figure 4. One month follow up.
