Findings:
The patient, who was paraplegic but otherwise healthy, was a non-smoker with a normal BMI. A grade IV pressure sore measuring 4x4x5 cm was present over the left tuber ischii, involving the bone, yet without significant undermining of the skin. The sore walls were fibrotic and had formed a chronic thick capsule. There were no signs of active infection observed either on the skin or in the wound status, and microbial swabs identified skin flora.

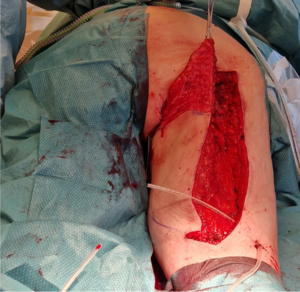
The ischial pressure sore stained with methylene blue to facilitate complete removal. A posterior thigh advancement flap has been outlined.
Treatment:
Under general anesthesia, the interior of the pressure sore was stained with methylene blue and then excised en bloc, leaving approximately a 2 cm margin between the wound wall and healthy, well-vascularized tissues. The exposed cortex of the tuber ischii at the base of the wound was removed using an osteotome (approximately 4 mm). Both the wound specimen and the bone were sent for microbiological assessment.

The resulting defect was larger than the skin opening and required additional padding (Figure 2). A random posterior thigh flap was incised according to pre-markings, initially to the level of the fascia. The muscle fascias were then meticulously released all around the flap, allowing for easy cranio-medial sliding. The flap reached the defect without the need for flap undermining or muscle division. The skin of the flap was deepithelialized to provide padding for the wound (Figure 3).
Parachute Vicryl 0 sutures were used to secure the padding to the periosteum/ligaments over the tuber ischii. Subsequently, the flap was sutured with Vicryl 2/0 at the level of the Scarpa’s fascia, subdermally, and finally with Ethilon 3/0 on the skin. The vertical incision was closed intradermally with Stratafix 3/0 sutures. Two active drains were inserted: towards the wound bed and under the distal part of the flap.

